
After Tess* was diagnosed with uterine fibroids, she discovered that there are plenty of treatment options to consider. This was great news. After all, many women are told fibroid surgery—such as a hysterectomy-—is their best option. In some cases, it is, but for others, non-surgical fibroid treatments could be equally, if not more, appropriate. Clearly, Tess had choices—but the more she researched, the more she realized how important it was to select the right one for her unique fibroid journey. More specifically, choose according to the type of uterine fibroids she had.
While it is easy to lump all fibroids under the same umbrella category, the reality is that there are four distinct types of fibroids, each defined by where they grow in or around the uterus. Simply put, where fibroids are located. That location can influence everything from symptoms and fertility concerns to even which fibroid treatment is most effective. While your doctor may have initially listed several possible fibroid treatment options—ranging from medication and minimally invasive procedures like Sonata, Acessa, and uterine fibroid embolization (UFE)—to hysterectomy and myomectomy, each option is not equally suited for every patient.
Understanding your fibroid type, location in the uterus, and which treatment options work best for those specific fibroids helps narrow the field. As a result, you and your physician can focus on the fibroid treatment most likely to provide meaningful, long-term relief. In turn, you will have peace of mind that you are taking control of your health needs.
Imagine Living Without These Uterine Fibroid Symptoms
- Heavy menstrual bleeding
- Abnormally long periods
- Intense cramps, pelvic pain, and pressure
- Bowel or bladder dysfunction
- Excessive fatigue
- Pain during sex
- Back or leg pain
- Weight gain or bloating
- Constipation, diarrhea, and rectal discomfort
Not All Uterine Fibroids Are the Same
Fibroids are non-cancerous growths that develop from the muscle tissue of the uterus. Most uterine fibroids are diagnosed in women between the ages of 35 and 54. However, fibroids can occur in women younger than 35 and until menopause. Depending on your situation, you may have one or several. But that does not mean they are all the same. One of the many characteristics of uterine fibroids is that they can differ in size and either remain the same size or grow at different rates. In many cases, they can range from the size of a pea or bean to that of a melon or grapefruit. According to the Office on Women’s Health (OWH), this is because estrogen and progesterone stimulate the development of the uterine lining during each menstrual cycle in preparation for pregnancy.
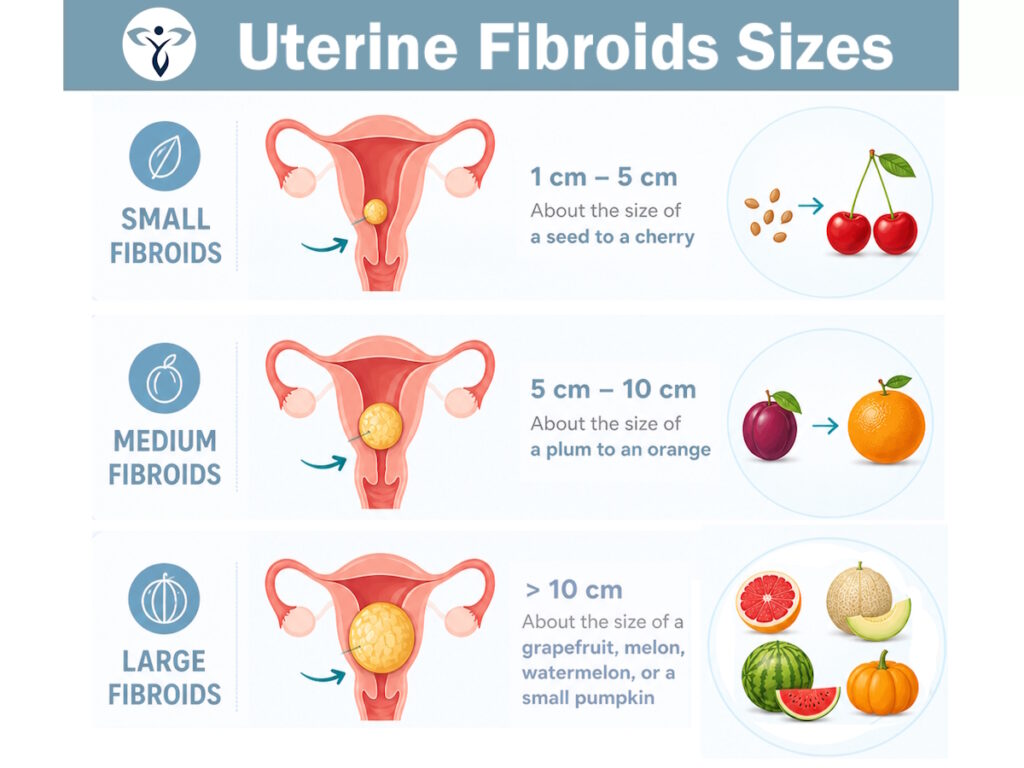
This causes fibroids to swell at different rates. So, you may have two or three fibroids, with two being the size of a melon and one the size of a small pumpkin. Here is a breakdown of what is considered a small or large fibroid.
- Small fibroids — Between 1 cm and 5 cm. Basically, the size of a small seed to a cherry.
- Medium fibroids — Between 5 cm and 10 cm. It can be the size of a plum to an orange.
- Large fibroids — Greater than 10 cm. The size of a melon, grapefruit, watermelon, or a small pumpkin.
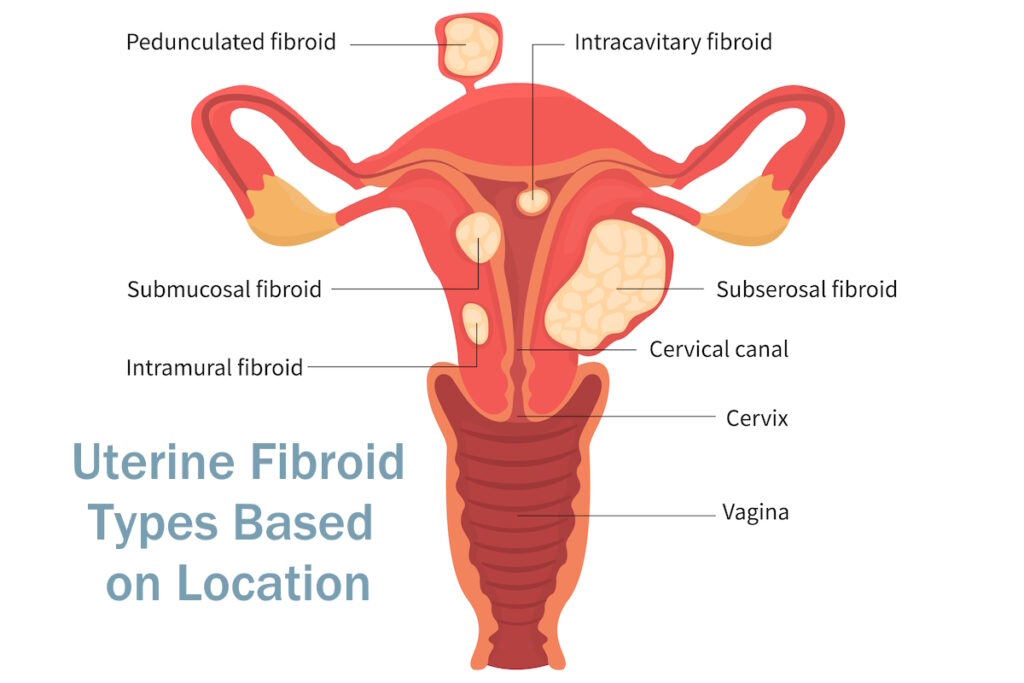
Location is also a major characteristic and the focus of this article. As previously mentioned, there are four types.
- Intramural fibroids — Grow inside the muscles of the uterine wall, causing issues with uterine function. Accounting for 70% of uterine fibroids, this is the most common, affecting one in four of all women of childbearing age.
- Submucosal fibroids — Protrude underneath the uterine lining and into the uterine cavity. Some women notice heavy bleeding during menstruation and increased abdominal pain from this type of fibroid.
- Subserosal fibroids — Tend to grow just outside the uterine walls, impacting surrounding organs. As a result, these can put pressure on the bladder, bowels, and abdomen.
- Pedunculated fibroids — Hang by a thin thread or stalk inside or outside the uterus. These are more likely to cause abdominal pain due to obstruction of the uterus and surrounding organs.
You can read more about each of these unique uterine fibroids in this article.
Why Fibroid Type Matters When Choosing Fibroid Treatment
Now that you understand the four types of uterine fibroids, the next logical question becomes: Which of the many treatment options you’ve been presented from your doctor or what you’ve read about online works best for each type? In our experience, this is where many patients tend to feel overwhelmed. A provider may mention options such as medications, myomectomy, hysterectomy, Sonata, Acessa, uterine fibroid embolization (UFE), or even endometrial ablation, but without understanding fibroid location, those options sound interchangeable. They aren’t.
Some fibroid treatments are designed specifically for fibroids inside the uterine cavity. Others work best for fibroids growing within the uterine wall or on the outside surface of the uterus. Choosing a treatment that does not align the fibroid type can lead to incomplete symptom relief, persistent bleeding, or the need for additional procedures later. Below is a simplified guide explaining how common treatments align with different types of fibroids.
Surgical Options
Hysterectomy — Roughly 600,000 hysterectomy procedures are performed annually in the U.S. It is a surgical procedure by which a doctor removes all or part of a woman’s uterus and, in some cases, her fallopian tubes and ovaries. A hysterectomy isn’t always necessary. In other words, advances in minimally invasive technology mean many women with uterine fibroids can choose options that preserve the uterus and offer faster recovery times and reduced surgical risks. That said, hysterectomy remains an effective and permanent solution.
This is true for all uterine fibroids—regardless of their size, number, or location in the uterus. Since the procedure removes the uterus and surrounding tissues, there is nowhere for fibroids to grow. New ones also can’t form.

Myomectomy — Similar to a hysterectomy, a myomectomy is another invasive surgical procedure for fibroid removal. The biggest difference is that the patient can keep her uterus. Your surgeon will carefully remove the fibroids one by one. Depending on how many fibroids are removed, your doctor may also need to reconstruct the uterus to maintain its strength and function. But does myomectomy work for all four uterine fibroid types? The answer to this question lies in the type of myomectomy procedure you and your doctor choose.
- Abdominal myomectomy: This version of the procedure allows your doctor more room to safely remove all fibroid types, including deeply embedded fibroids and those that are excessively large or in large quantities. However, the tradeoff is that it is far more invasive than other myomectomy procedures, as it requires a long incision in the lower abdominal region and in the area of the uterus where the fibroids are located.
- Laparoscopic myomectomy: This is less invasive in comparison because it only requires four tiny incisions to access the uterus, but it is not ideal for removing fibroids that are deeply embedded. It is best suited for intramural fibroids and subserosal fibroids.
- Hysteroscopic myomectomy: An outpatient procedure, hysteroscopic myomectomies are only appropriate for patients whose fibroids are located in the uterine cavity (submucosal). Given the ease of access, your surgeon will use a thin, telescopic tube to access the uterine cavity before lifting the uterine walls to shave off the fibroids.
Even though hysterectomy and myomectomy procedures are both popular and effective, there is the possibility that a woman is not a good candidate for surgery. For instance, she may have other health conditions, such as uncontrolled diabetes or heart disease, that increase surgical risk. She might have a history of severe abdominal or pelvic scarring that makes surgery more complicated. She could also be at higher risk for blood clots or infections.
Beyond not being a good candidate, many women simply do not want to undergo a bloody surgical procedure. While effective, these procedures carry significant risks and require hospital stays and lengthy recovery times. There is also the reality that pregnancy may not be an option with a hysterectomy.
This is where non-surgical options can be highly viable considerations.

Non-Surgical Options
Medications — Certain medications, such as gonadotropin-releasing hormone (GnRH) agonists, non-hormonal medications like tranexamic acid, or NSAIDs, can help control bleeding and pain without surgery. And yes, they will work across all fibroid types. That said, the fibroids do not go away. Therefore, if you stop taking the medicine, symptoms can return. In some cases, symptoms may worsen.
Uterine Fibroid Embolization — UFE is a revolutionary, advanced procedure that has become the gold standard for non-surgical fibroid treatment. Why? For starters, since it is not surgery you can go home the same day. More importantly, it works on all fibroid types—regardless of size and location. All fibroid types can be treated. Rather than removing fibroids with numerous incisions, UFE cuts off blood flow to all fibroids. UFE is low risk, has no incision, is faster than other options, and is one of the top reliable ways to treat fibroids. If a woman is not eligible for UFE, there are other options to consider.
Acessa — The benefit of this procedure is that it heats and destroys fibroids rather than physically removing them. But there are limitations given that Acessa approaches fibroids from outside the uterus. For example, if you have multiple large fibroids (melon- or grapefruit-sized) or fibroids that are hard to reach or in high-risk areas, such as those in the cervix, Acessa is not a good choice. Acessa is best suited for intramural and subserosal fibroids. In some cases, it can help with submucosal and pedunculated fibroids.
Sonata® System — This incisionless fibroid treatment works well for patients with one or several fibroids. Using an intrauterine ultrasound device, radiofrequency energy is delivered to the fibroid to shrink it. As the fibroid shrinks, the patient can see a reduction in painful symptoms. That said, ideal fibroids for this approach are those within the uterine cavity (intramural and certain submucosal fibroids).
Endometrial ablation — This is a slightly different procedure, as the goal is to treat the uterine lining and reduce heavy bleeding rather than the fibroids themselves. This procedure can still be effective for small submucosal fibroids that are directly contributing to heavy bleeding but using it for other types will likely lead to less-than-ideal results for long-term relief.
Fibroid Institute Offers Revolutionary Fibroid Treatment. Let’s Talk Today!
If you’ve been diagnosed with uterine fibroids, a comprehensive evaluation can help determine which treatment is most likely to relieve symptoms while aligning with your health goals and lifestyle. These are the in-depth conversations you will want to have with your primary care physician or gynecologist. Whether UFE is the right option for you or not, our team of fibroid doctors is always on hand to partner with you and your PCP or OBGYN to determine the best course of action.
If uterine fibroid embolization (UFE) is your preferred path, the only decision remaining is to select the right interventional radiologist for UFE care. Beyond the procedure itself, women want an experienced fibroid doctor who provides access, communication, comfort, innovation, trust, and a supportive experience from start to finish. The Fibroid Institute is here to offer you just that.
In addition, we simplify your UFE journey, managing everything from insurance to PCP communication while providing all patients with direct access to their fibroid doctor before and after their procedure. Our physicians are board-certified interventional radiologists and experts passionate about helping women become #FibroidFree. The bottom line is that you do not have to worry about ongoing challenges of missing work and life events with UFE as your fibroid treatment procedure.
Becoming Symptom Free Is As Easy as one, two, three …

At the Fibroid Institute, we do not believe you need to decide between suffering in silence and having invasive surgery. With multiple locations, our fibroid clinics help thousands of women avoid fibroid surgery and find relief from their fibroid symptoms. Meet some of these women here:
Our fibroid doctors are board-certified interventional radiologists, highly experienced UFE specialists, and experts passionate about helping women become #FibroidFree. Request a free 10-15-minute phone screening to determine if you are eligible. If you qualify for UFE after the screening, you can schedule your on-site or telehealth consultation. Most major medical insurance providers cover the cost of UFE.
Get started now by calling our Dallas, Texas clinics at 214-838-6440, Houston, Texas clinics at 713-903-3733, South Carolina clinics at 843-628-4290 or complete the form below.
"*" indicates required fields
This information is not a substitute for professional medical advice. Prior to starting any new treatment or if you have questions regarding a medical condition, always seek the advice of your doctor or other qualified health provider.
The Fibroid Institute serves the Charleston, South Carolina, Dallas/Fort Worth, Texas and Greater Houston, Texas metro areas including Addison, Allen, Arlington, Bedford, Bellaire, Carrollton, Cedar Hill, Charleston, Clear Lake, Cockrell Hill, Conroe, Craig Ranch, Cypress, Dallas, DeSoto, Duncanville, Euless, Fort Worth, Frisco, Garland, Grand Prairie, Highland Park, Houston, Hurst, Hutchins, Irving, Katy, Kingwood, Lancaster, League City, McKinney, Mesquite, Mt. Pleasant, Murrells Inlet, Orangeburg, Park Cities, Plano, Richardson, Sherman, Spring, Stafford, Sugar Land, Summerville, Texas City, The Woodlands, Universal City, University Park, Walterboro, Webster and more.
*Patient names and/or photos may be changed to protect patient confidentiality.